Well...it isn't exactly known.
The functional causes are easier to focus on:
(1) Is there a history of trauma?
(2) Is there a history of disease (including low grade inflammation)?
(3) Is there an abnormal movement system or motor control placing stress on the nervous system?
Keep in mind, if 1 & 2 are present, it doesn't mean that movement still isn't placing stress on the nervous system.
Some simple tests can give us the answers.
Want to Learn?
We are doing this course in Calgary, Alberta Canada Dec 13-15, 2019 (2pm Friday start)
Course Description
The nervous system may become
reactive and sensitized through many processes. One such process is
through abnormal movement patterns. On this course the base neurodynamic
tests are reviewed we will show how correcting movement patterns can influence
neurodynamic reactivity. Examples will be highlighted where movement
control rehabilitation and neurodynamics do not agree i.e. when the ideal
movement pattern actually places more stress on neural structures.
This course will provide
participants with skills in analysing movement in relation to neurodynamic
reactivity. Specific motor control retraining strategies will be introduced
using a comprehensive and clinical reasoning process.
Strategies will also be covered to
combine traditional neural mobilization with motor control exercise.
The course will cover the neck and
upper quadrant as well as the trunk and lower quadrant.
Course Objectives: The participant will be able to:
- Understand how uncontrolled movement patterns and poor
motor control may contribute to reactivity of the nervous system
- Use motor control retraining strategies to treat
neurodynamic reactivity
- Understand when normal movement can aggravate sensitive
neural tissue and problem solve to use other techniques
- Use movement pattern control rather than time
frames as a predictor of outcome
WHAT WILL YOU GET THAT YOU MAY NOT
ALREADY HAVE?
How do you mobilize the nervous
system and control movement? How do you use to unload the nervous We'll show you!
How do you rehab the Slump Test when
there is also excessive Lumbar Flexion? There
does not seem to be a logical way to rehab both of these problems. We'll show
you how!
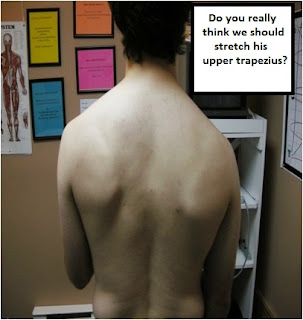
The ideal scapular position can
change when neurodynamics is present
Based on anatomy, biomechanics,
motor control and clinical research we have an ideal scapular position this can
change when neurodynamic reactivity is present – hence what we think is good
rehab can be harmful some people
Upper Trapezius is a Good Muscle –
find out why!
Taping
There are some great taping
techniques for shoulder girdle, forearm and neurodynamic problems.
Neck rehab is so much more than the
Deep Neck Flexors! In the deep neck flexors when
neurodynamic reactivity is present frequently aggravates symptoms.
Popliteus is one of the missing links in of anterior knee pain and
lower limb dysfunction. What does it do? How do we retrain it?
Why Do We Move Differently?
We'll review some key Primitive
Reflexes that are involved in neurodynamics and discuss the known mechanisms of
altered movement.
Testimonials
“I can't recommend Sean Gibbons and
Smarterehab courses enough. I have found the sub-classification system to be
easy to use and revolutionary in removing a lot of the guesswork in my patient
management. The courses have been transformative in my practice in that it
has wide applicability across a spectrum of conditions that would normally
constitute ‘difficult’ patients. I can't recommend these courses highly enough!Chris Barber MCSP BSc (Hons) Musculoskeletal
& Sports Physiotherapist, Director: Advanced Physiotherapy Centres Ltd.
As a clinic owner and have seen a
trend in Canadian physiotherapy towards spinal manipulation and needling
techniques. While these techniques are valuable, the transformative learning
that takes place in a SmarteRehab course is the direction I am dedicated to
bringing our profession. As Physiotherapists, if we wish to distinguish
ourselves from chiropractors, massage therapists, athletic therapists,
osteopaths etc., we need to move away from technique based therapy. Sean is
masterful at explaining the complex relationship between Central Sensitization,
Central Pain, Sensori-Motor Function and how it relates to Motor Control
dysfunction and pain. No other approach I have seen, heard of, or even read about
does such a complete job of integrating neurological rehabilitation techniques
and orthopaedic treatment. I now have junior therapists who are able to reason
their way through the most complex of chronic pain cases and can formulate
treatment plans that are effective and get results. Most importantly they can
explain to these patients the nature of their problem in a way that they can
understand. It is so rewarding to see patients, empowered with this
knowledge, resolve problems that have sometimes existed for decades.
Equally as rewarding is watching a junior Physio quickly solve an orthopaedic
complaint by identifying the underlying movement dysfunction and easily
explaining it’s cause. Thank for what you have done and continue to do for our
Profession.Dave Holmes Owner
and Physiotherapist at Tower Physiotherapy & Sports Medicine
If you find yourself stuck and
frustrated with chronic, generalized, weird pain patients who don't respond to
usual treatments, this is what this course is all about. Sean's courses are
truly unique and bring practical, guidelines that are untouched by other
institutions. Places are limited.
Testimonial- Pelvic Floor Therapist
The courses that I have taken with
Sean have completely changed my pelvic floor practice and the way I practice as
a physical therapist! Sean's courses are a must in order to help a variety of
clientele and especially those who do not respond to conventional
treatments! He has researched and developed new techniques that are
essential for pelvic floor therapists.
Erica Lafontant, pht, B. Sc, M.Sc.A
Rééducation périnéale et
Action Sport Physio
Ville Mont-Royal, QC,
Facilitator
Sean Gibbons graduated from
Manchester University in 1995. He has been rehabilitating movement patterns for
over 20 years. He is an international expert in specific motor control exercise
and has researched and developed numerous advances the cognitive control
of movement to make the rehab process better. These include predicting who can
learn, understanding who can learn but will not respond, and integrating which
postural and primitive reflexes influence movement and key aspects
neurodevelopment. His PhD was on the development of a prescriptive clinical
prediction rule for specific motor control exercises in low back pain. Key new
sub-classifications were identified: Neurological Factors, which are related to
poor movement and the ability to learn; Midline as a sensory system which is
critical to Body Image Pain; and Neuro-Immune dysregulation, which is critical
for Central Sensitization and Psychosocial Factors. His current work involves
further researching the sub-classification model. His dissection and research
into psoas major, gluteus maximus and other muscles led to the development of
new rehabilitation options. He has presented his research at national and
international conferences and has several journal publications and book
chapters. He is an Assistant Clinical Professor (Adjunct) at McMaster's
Advanced Orthopaedic Musculoskeletal / Manipulative Physiotherapy
specialization and lectures at Manchester Metropolitan University's Masters in
Advanced Physiotherapy program.